Irvine, California, where health insurance premiums for the average 25-year-old who purchases insurance for himself will nearly double under Obamacare. (Photo credit: Wikipedia)
Well, it’s been an interesting week in health care land. For a while now, independent analysts—and conservative critics—have raised concerns that Obamacare will dramatically increase the cost of individually-purchased health insurance for healthier people. This would, of course, contradict President Obama’s promises that “if you like your plan, you can keep it” and that the cost of insurance would go down “by $2,500 per family per year.” What’s new is that liberal columnists, facing reality, are conceding that premiums will go up for most people in the individual market. But they’re justifying it by saying that “rate shock” will help a tiny minority of people who can’t get insurance today. If they had said that in 2009, would Obamacare have passed?
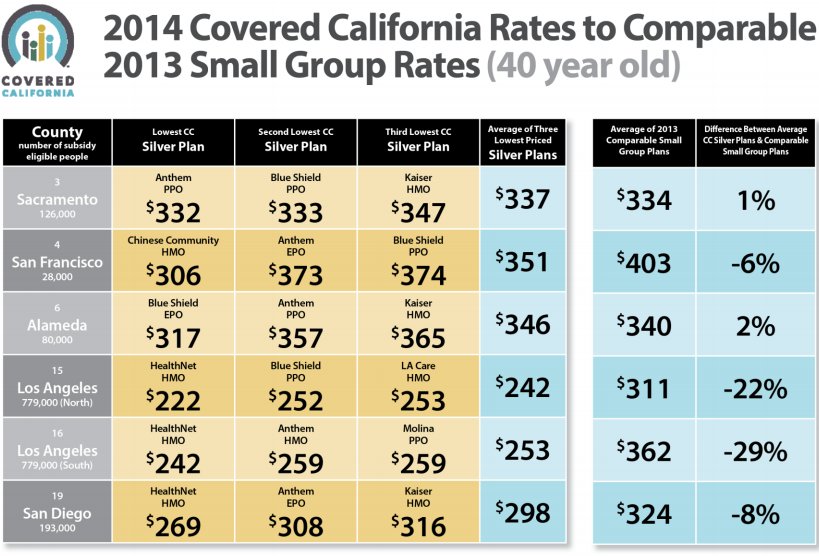
Last month, progressive pundits were trumpeting news out of California that the cost of health insurance under Obamacare in that state was surprisingly low. “Well, the California bids are in,”
wrote Paul Krugman on May 27. “And the prices, it turns out, are surprisingly low…So yes, it does look as if there’s an Obamacare shock coming,” the shock that Obamacare will work just fine.
It turns out, however, that Krugman was uncritically regurgitating California’s misleading press release. In fact, the average 25 and 40-year-old will pay double under Obamacare what they would need to pay today, based on rates posted at
eHealthInsurance.com (NASDAQ:
EHTH). More specifically, for the typical 25-year-old male non-smoker, the average Obamacare “bronze” exchange plan in California will cost between 64 and 117 percent more than the cheapest five plans on eHealth. For 40-year-old male non-smokers, it’s between 73 and 146 percent more.
Democrats now: It’s ok if premiums double for average people
Ezra Klein of the
Washington Post, in
response to my
article on this topic, checked out the eHealth rates for plans in his hometown of Irvine, California, and compared them to a similar website sponsored by the government at healthcare.gov. He found that the third-cheapest plan there cost only $109 a month, “if they’ll sell it to you for that price.” According to the government, Ezra notes, 14 percent of people who tried to buy that plan—Health Net’s IPF PPO Value 4500—were turned away. Another 12 percent were asked to pay more than $109.
To Ezra, it’s galling that three-fourths of his compatriots can pay $109 for health insurance, because 12 percent were not eligible for the plan, and another 14 percent had to pay somewhat more. This is why Obamacare is a great achievement, he says, because Health Net will have to serve all comers, regardless of prior health status.
And I appreciate Ezra’s perspective. I, too, am a
supporter of universal coverage, so I understand Ezra’s passion for providing health insurance to the sick. But what we didn’t know last week—and we do now—is
how much more the healthy will have to pay for that insurance, under Obamacare. In Orange County, where Irvine is located, the three-fourths of the 25-year-old population that is in good health will have their premiums jacked by 95 percent.
And that’s for Obamacare’s “catastrophic” coverage; the more comprehensive “bronze” plan increases premiums by 130 percent. For the fraction—one-eighth of the total—who, under the old system, would have been charged more, the premium increase due to Obamacare will be somewhat less.
And the vast majority of those who were turned away are able to find insurance—albeit at a higher price—elsewhere.
Based on enrollment in Obamacare’s
high-risk pool program, the number of people in America who are truly uninsurable is closer to 150,000. That’s a pretty small number in a nation of 300 million. Previous estimates of the uninsurable population came in around 2 to 4 million people, but it’s likely that for many of these individuals, the principal problem is not that they’re denied coverage, but that the premiums are high.

Experts in the economics of health insurance understand that this has been Obamacare’s central flaw
from the beginning. The law’s heavy-handed approach to the health insurance market
massively drives up premiums for the average person.
Ezra makes another accurate point that is important to emphasize: these increased premiums affect people who shop for insurance on their own. If you get insurance through your employer, especially if your employer is large, you should be significantly less affected. But an increasing number of people shop for insurance on their own, because fewer and fewer employers are sponsoring health coverage.
According to the Congressional Budget Office, in 2022, around 25 million people will be purchasing coverage for themselves, and another 25 million will be enrolled on the exchanges. That’s a lot of people. And it doesn’t include the 30 million that will remain uninsured.
Universal coverage,
done right, can address these problems in a way that makes insurance affordable for everyone. But Obamacare’s sops to special interests—from the various services all plans are required to cover, to the fact that the law forces young people to pay more to subsidize well-established older people—is not the right way, because it makes insurance too costly.
Democrats then: Rate shock is a right-wing myth
The key thing to remember is that back when Obamacare was being debated in Congress, Democrats claimed that it was right-wing nonsense that premiums would go up under Obamacare. “What we know for sure,” Obamacare architect Jonathan Gruber
told Ezra Klein in 2009, “is that [the bill] will lower the cost of buying non-group health insurance.”
For sure.
In 2009, was Ezra saying that it’s ok that premiums will double for the average person, because a minority of people will pre-existing conditions will benefit? No.
Earlier that year, AHIP, the private insurer trade group, commissioned a
report from PriceWaterhouseCoopers to analyze the impact of Obamacare on health insurance premiums in the individual market. That report, which I
reviewed here and
elsewhere, found that the version of Obamacare then being considered by the Senate Finance Committee would increase premiums by 14 to 32 percent, depending on the year you looked at. In retrospect, the PwC report was a bit optimistic.
But Ezra
described the PwC analysis as “the insurance industry’s deceptive report,” comparing it to sham research put out by the tobacco industry and Big Oil. Ezra did concede at the time that “buying better insurance will cost somewhat more,” because insurers would no longer be able “to sell a deceptive and insufficient product.”
But high-deductible, catastrophic insurance isn’t cheaper because it’s dishonest. It’s cheaper because it’s more efficiently designed. And it’s precisely that sort of efficiently-designed insurance that Obamacare abolishes.
Businesses in competitive markets can’t survive by cheating
This idea that high-deductible insurance, freely purchased in a voluntary exchange, is a “dishonest” product is an article of faith in some quarters. My good friend and
Forbes colleague Rick Ungar recently dedicated an
entire blog post to the subject. The numbers that come out of eHealthInsurance.com, Rick says, are lies. What data does Rick cite to prove this? He doesn’t cite any actual numbers. Instead, he cites…anonymous reviews on the internet.

Rick went to epinions.com, and pulled out quotations from people who were unhappy with eHealth’s customer service. And eHealth should certainly do what it can to address customer’s complaints. (The company, however, isn’t directly responsible for the customer service of the insurers whose products it sells.) Remember that, unlike with Obamacare, eHealth is a private business. No one is forced to use their services. Those who do have a bad experience on eHealth can go elsewhere, like healthcare.gov. eHealth, unlike the government, has an economic incentive to make its customers happy. Indeed, the default setting at eHealth is to sort the listed plans by customer popularity.
If we abolished every company with negative reviews on the internet, we wouldn’t have much of a private sector left. But that’s effectively Rick’s—and Obamacare’s—logic. Once the Obamacare battle station becomes fully operational, eHealth won’t be allowed to sell inexpensive insurance plans. Everyone will pay the higher rate, the higher rate that Rick Ungar’s commenters once thought was a bad deal.
And if we go to a site equally as reliable as epinions.com—my
comments section—we find a much more revealing assessment of eHealth’s business practices. Commenter Robert W. says that, because he has a pre-existing condition, the insurer in Georgia who listed a plan costing $130 a month on eHealth charged him $260 instead. Unsurprising. But several other commenters weighed in to say that they had had positive experiences on eHealth.
Commenter Steve Getman: “That wasn’t my experience when purchasing coverage from eHealthInsurance 3 years ago. The rate I ended up paying was the same as the quote.”
Walt Kienzle: “I had a quite different experience [from Robert W] with Blue Cross Blue Shield of Illinois. I was quoted $97 per month for my premium and that is exactly what I have paid for the past year. My policy is paid up until December, so they can’t change the rate until then. When a friend of mine who is also 51 needed to buy her own coverage, I pointed this policy out to her. She has rheumatoid arthritis and gets the same rate.”
Joseph Scott: “As a 26 year old male in San Francisco, I now pay $137 per month for medical insurance and $26 for dental on an independent plan. Using the CoveredCA site, my anticipated OBAMACARE premium, for a less desirable plan, will increase to $203 per months; not including dental.”
Johnny Heedless: “Like many others, what you’re describing is certainly not my experience. I currently purchase my insurance through ehealthinsurance.com I pay EXACTLY what I was quoted.”
There’s more where those came from. And needless to say, Rick didn’t talk about the quality of customer service under Medicaid, or other government agencies like the IRS, that Obamacare substantially expands to achieve its ends.
It’s true that, if you have a pre-existing condition and you don’t put it on your application form, the insurer will call you out for it, and charge you more. They don’t do this because they’re mean. They do that because
insurers would go broke if they charged people less than the cost of their care. You can’t buy car insurance after you’ve crashed your car, or homeowner’s insurance after your home has burned down, without paying a higher price, for the same reasons.
There is a better way
I wholeheartedly agree that we should do something to help the small number of people with pre-existing conditions who genuinely can’t obtain insurance. There’s a better way, as Doug Holtz-Eakin and I
explained here. It’s important to remember that the problem is an artificial one, created by
World War II-era wage controls and a series of other unwise government policies.
Simple changes to Obamacare, like repealing the law’s requirement that
young people pay similar premiums to old people, and relaxing its constraints on deductibles and co-pays, would help reduce rate shock. But Democrats put “community rating” in the bill in order to please their allies in the AARP, and many on the left are ideologically opposed to high-deductible insurance. These provisions have a lot to do with rising premiums under Obamacare, and removing them doesn’t prevent you from covering those with pre-existing conditions.
An argument you hear from the left is that it’s no big deal that Obamacare hikes premiums, because poor people won’t have to pay those prices; their plans will be subsidized by the government. But this is an economically and fiscally irresponsible point of view. We’re going to make health insurance unnecessarily expensive—thereby placing an extra burden on taxpayers and those ineligible for subsidies—and it’s no big deal because the government will
insulate a select few from the costs?

The fact that Obamacare dramatically raises premiums on young people is a big deal, because the majority of uninsured people are young. It’s the fact that insurance is already so expensive that leads so many young people to opt out. They’re perfectly healthy; they don’t have a lot of money; but they’re being asked to shell out thousands of bucks for policies they won’t use. And Obamacare’s solution to this problem is…to force them to pay more? We’ll see how that goes.
But in the end, I’m glad that we’re finally having the intellectually honest argument about Obamacare that we should have been having all along. No, Obamacare won’t decrease the cost of your insurance by $2,500 a year. Indeed, it could raise it by that much. No, under Obamacare, you can’t keep your plan, if you like your plan. Instead, you’ll be forced to buy a costlier plan with add-ons that you neither need nor want.
If you’re a leftie, you likely think that’s a good thing. But you should have said so all along. The fact is that Obamacare was sold to the public under false pretenses, and the chickens are now coming home to roost.











")


